Assistant Professor, Icahn School of Medicine at Mount Sinai
Test the abil- r Bradykinesia (slowness in movements) is noticeable ity of the patient to sit on the edge of the bed with their when doing alternate hand tapping movements blood pressure chart mayo generic 100 mg furosemide overnight delivery, or arms crossed heart attack quick treatment order generic furosemide on line. Micro- r Gait:Wide-basedgait blood pressure medication safe for pregnancy generic furosemide 40mg with amex,withatendencytodrifttowards graphia (small, spidery handwriting). Even a mild cerebellar problem makes tiation of movement is impaired (hesitancy) with the this very difcult. A festinating gait is Causes include the following: r when the patient looks as though they are shufing in Multiple sclerosis r order to keep up with their centre of gravity, and then Trauma r has difculty in stopping and turning round. The three groups of tremor are distinguished by obser- r Metabolic: Alcohol (acute, reversible or chronic de- vation (see Table 7. If unilateral, the leg is swung out to the side to move it forwards (circumduction). If bilateral, the Extrapyramidal signs (Parkinsonism) pelvis has to alternately tilt and the gait often becomes r Appearance: Expressionless face. Thepatientcanstandontip-toe,butoften Resting tremor which is slow and classically pill- not on their heels. Even if mildly affected the patient is unable to strating whether seizure activity is suppressed by walk heel-toe in a straight line. In or encephalitis, as well as occurring in focal status Parkinsons disease, this pattern tends to be asym- epilepticus. They are useful in the di- agnosis of muscle disease, diseases of the neuromuscular Electroencephalography junction, peripheral neuropathies and anterior horn cell disease. It is obtained by placing electrodes on the scalp, using a jelly to reduce electrical Electromyography resistance. A recording of at least half an hour is usually Aneedleelectrodeisplacedintomusclesandinsertional, needed, to maximise the chances of picking up tran- resting and voluntary electrical activity is studied, using sient abnormalities. Its main use is for the classication of epilepsy, but is r Peripheral neuropathies and anterior horn cell disease it may also be useful in the diagnosis of other brain dis- lead to a reduced number of motor units, which re orders such as encephalitis. Surface electrodes or occasionally needles are used both r Suspected spinal cord compression. The knees are drawn up as far as possible and uation of brachial and lumbosacral plexus and nerve the neck exed, to open up the spinous processes of the roots. The lumbar puncture needle is inserted in the midline Lumbar puncture with its stylet in place aiming slightly towards the um- bilicus. If the needle encounters rm resistance, it Indications should be withdrawn and another approach tried. When any of the following are suspected: Sometimes the patient will feel a pain radiating into r Infection (meningitis, encephalitis, fungal infections the leg or back this is due to the needle touching a or neurosyphilis). A simultaneous blood diagnosis of idiopathic (benign) intracranial hyperten- sample for glucose should be sent. Thereisadiffer- in the case of sick patients, is relatively unaccessible ence in healthy tissue and infarcted, infected or oedema- although some units have facilities for ventilation in the tous tissue. Cerebrovascular disease Faster scans are now possible particularly helpful for patients unwilling or unable to lie at for long, although in some cases general anaesthetic may be necessary for Stroke unco-operative patients. Magnetic resonance imaging uses the magnetic proper- ties of protons to generate images of tissues. It has the advantage of not exposing the patient to ion- Incidence ising radiation (particularly important in young infants, Third commonest cause of death in Western World (12 childrenandpregnantmothers). Geography Posterior circulation (the vertebral, basilar arteries and Black community, Japanese more common. They are predisposed to by hypertension and diabetes, are often asymptomatic but may cause focal neurologi- Pathophysiology cal defects such as weakness of a single limb, or limited Haemorrhagic strokes are discussed elsewhere. The nal picture may affected, and whether there is temporary or permanent include dementia and a shufing gait which resembles ischaemia and hence infarction.
M > F Age Pathophysiology Bimodal distribution with a peak in young adults (1534 Although there is a proliferation in B cells they have years) and older individuals (>55) blood pressure medication buy generic furosemide from india. On Aetiology examination there may be lymphadenopathy and hep- Infectious agents particularly Epstein Barr virus have atosplenomegaly hypertension bp order 100mg furosemide amex. Involvement with intermittent chemotherapy such as chlorambucil of mediastinal lymph nodes may cause cough prehypertension pediatrics buy line furosemide, shortness or udarabine. B symptoms may be present (fever >38C, drenching night sweats, weight loss of Prognosis more than 10% within 6 months). The staging of Hodgkinss disease is accord- ing to the Ann Arbor system, which is sufxed by B if Chronic myelogenous Leukaemia Bsymptoms are present and A if they are absent (see See Myeloproliferative disorders page 482. Microscopy Non-Hodgkins lymphoma Classical Reed-Sternberg cells are large cells with a pale cytoplasm and two nuclei with prominent nucleoli said Denition to resemble owl eyes. Incidence r Mixedcellularity disease which mainly affects older 20 per 100,000 per year. Tumours arise due therapy or a combination depending on the stage of to multiple genetic lesions affecting proto-oncogenes Table12. Clinical features r Indolent: Most patients present with painless slowly Prognosis progressive lymphadenopathy. Lymph nodes may re- Indolent lymphomas have a predicted median survival duce in size spontaneously making it difcult to dis- time of 510 years. B symp- sponsive to chemotherapy but have a predicted median toms (fever >38 C, drenching night sweats, weight survival 25 years. On Paraproteinaemias examination there is lymphadenopathy and hep- atosplenomegaly. The cells are trophic to the skin particularly the hands and feet, and result Age in plaques and lumps of associated with generalised Most commonly diagnosed 6065 years. Gas- trointestinallymphomaisparticularlycommoninthe Pathophysiology MiddleEastandisalsoseeninassociationwithcoeliac There is expansion of a single clone of plasma cells that disease. Cleavage of these immunoglobulins tribution according to the Ann Arbor system, which result in the production of Fab and Fc fragments; the Fab is sufxed by B if B symptoms are present (see fragment is termed the Bence-Jones protein and is found Table 12. Investigations There is also production of osteoclast stimulation fac- Thediagnosisismadebylymphnodebiopsy,cytogenetic tor causing lytic bone lesions, bone pain and hypercal- studies of lymphoma cells may give prognostic informa- caemia. Spinal cord compression occurs in approx- imately 1020% of patients at some time during Pathophysiology the course of disease. Hypercalcaemia causes thirst, The abnormal proliferation of lymphoplasmacytoid polyuria, constipation and abdominal pain. Investigations The diagnosis of myeloma is made if there are: Clinical features r Bone marrow aspirate has at least 1015% plasma Hyperviscosity presents as weakness, tiredness, confu- cells. Patients also often have peripheral lymphadenopa- Other investigations include: thy. Chemotherapy with single alkylating agents improves r Protein electrophoresis shows an IgM parapro- prognosis. Recently, thalidomide has been demonstrated to produce a signicant response Management in 30% of patients whose disease progressed following Chemotherapy produces a variable response. Supportive care includes blood transfu- pheresis is used for symptomatic hyperviscosity. Investigations Sex Electropheresis of serum protein demonstrates a raised X linked; males only affected. Aetiology Mutations on the X chromosome including deletions, Management frame shifts and insertions.
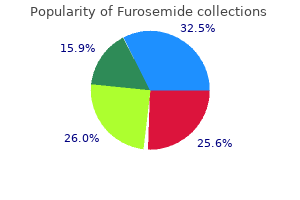
Buy furosemide 100mg amex. Most Popular Acupressure Points for Self Treatment.
Measurement of the lecithin/sphingomyelin ratio and phosphatidylglycerol in amniotic fluid: an accurate method for the assessment of fetal lung maturity hypertension updates quality furosemide 40mg. Comparison of performance of various sphygmomanometers with intra-arterial blood-pressure readings hypertension quality improvement order furosemide 40 mg. Comparison of clinic and home blood-pressure levels in essential hypertension and variables associated with clinic-home differences arteria carotida interna effective furosemide 40mg. Statistical comparison of multiple analytic procedures: application to clinical chemistry. Comparison of the new miniature Wright peak flow meter with the standard Wright peak flow meter. By promoting the right dosage of physical activity, you are prescribing a highly effective drug to your patients for the prevention, treatment, and management of more than 40 of the most common chronic health conditions encountered in primary practice. This Guide acknowledges and respects that todays modern healthcare provider may have only a brief window of time for physical activity counseling (at times no more than 20-30 seconds) during a normal office visit. Refer your patients to certified exercise professionals, who specialize in physical activity counseling and will oversee your patients exercise program. The Physical Activity Assessment, Prescription and Referral Process documents are the core of the guide and will explain how you can quickly assess physical activity levels, provide exercise prescriptions, and refer patients to certified exercise professionals. Print out and display copies of the Office Flyers in your waiting room and throughout your clinic. Regularly assess and record the physical activity levels of your patients at every clinic visit using the Physical Activity Vital Sign. For patients with chronic health conditions, the Your Prescription for Health series will provide them with more specialized guidance on how to safely exercise with their condition. Once you are comfortable with the prescription process, begin referring your patients to local exercise professionals who will help supervise them as they fill their physical activity prescriptions! These steps are all described in greater detail throughout the rest of this Action Guide. Keep reading to find how you can make a difference in getting your patients to be more physically active! In contrast, physical inactivity accounts for a significant proportion of premature deaths worldwide. As a healthcare professional, you are in a unique position to provide such expertise to your patients and employees in helping them develop healthy lifestyles by actively counseling them on being physically active. The first step you can take within your healthcare setting is to ensure that you walk the talk yourself. Data suggests that the physical activity habits of physicians 1 influence their counselling practices in the clinic. To be a role model for your healthcare team and to gain the trust of your patients, an important first step is setting an example and showing that being physical active is important to you! Next, we encourage you to focus on the well-being of your healthcare team and implement steps that will increase their physical activity levels and healthy lifestyle choices. Some of these steps may include: Implementing wellness challenges and programs Offering physical activity classes (i. Finally, we strongly encourage you to promote physical activity in your clinic setting. You may not always have time to engage your patient in conversations about their physical activity levels, but there are simple steps that you can take to make sure they realize its importance in their personal health.
Aspirin (blocks thromboxane production preferentially make prostacyclin) blood pressure chart in spanish order furosemide once a day, antihypertensives prehypertension need medication order furosemide 40mg with visa, anticonvulsant prophylaxis (Magnesium sulphate) heart attack radio edit purchase furosemide pills in toronto. Have to stabilise before delivery Delivery is the only cure (although > half of fits occur post partum). Bleeding from an abnormal fetal vessel attached to the membranes over the internal os. Monitor retro-placental clot by serial ultrasound Rhesus haemolytic disease* Aetiology: if Rhesus ive mother is contaminated by blood from a Rhesus +ive baby anti-D IgG antibodies (isoimmunisation) Later in the pregnancy, or in a following pregnancy, IgG can cross the placenta causing Erythroblastosis Fetalis ( stiff oedematous lungs and hydrops widespread oedema) nd Test for anti-D antibodies in all Rhesus ive mothers at booking and in 2 trimester. Hard to diagnose regular uterine contractions are normal, cervical changes in labour can be subtle Braxton-Hicks contractions are usual from 30 weeks but are not painful History: Is it true labour: check nature of contractions, urinary frequency (? Can risk of infection Steroids: dexamethasone and betamethasone (crosses placenta, prednisone doesnt) - 2 shots 12 hours apart. Epidural analgesia preferable to narcotics ( respiratory depression) Reproductive and Obstetrics 367 Premature Rupture of Membranes* = Rupture of membranes before labour is established. Normally rupture of membranes follows establishment of labour Check: have they really ruptured? Continuous monitoring interventions) Intermittent auscultation every 15 30 minutes following a contraction. Only worry after 36 weeks it can turn fairly easily before then Transverse or oblique (1%) Fetal Attitude: posture of the fetus, eg extended neck Fetal Position: Relation of occiput (vertex) to the maternal pelvis. If engaged, you know the pelvic inlet is big enough Descent: Extension of fetal body. Usually descent through pelvis transverse, then need to rotate face downwards Extension: once head reaches vulva, occiput in direct contact with symphasis. Ritgen Manoeuvre upward pressure on chin through perineum from below, downward pressure on occiput (stop anterior tear) External Rotation/Restitution occiput goes back to original position (transverse) now realigned again with shoulder. Check for nuchal cord (around neck), clear nasopharynx Expulsion: anterior shoulder, followed by posterior shoulder. Gentle traction on chord with supra-pubic pressure (stops uterus coming down) or fundal massage and maternal bearing down without traction Can manually deliver (place hand into uterus and separate) if no haemorrhage then wait for anaesthesia Then inspection, repair, rectal exam Cord prolapse: Cord comes through cervix before head. During active stage, progress = either further dilation or further descent Can happen at any stage Causes of failure to progress: Prolonged latent phase Primary dysfunctional labour: never enters active phase. C-section if < 1000 gm (body comes through at 7 8 cm dilated and head gets stuck = entrapment of after-coming head) or > 3600 or 4000 gm. C-section becoming more routine for any breech Face (rather than occiput first). Converts to either face or occiput cant deliver as brow Occiput transverse: Head cant flex and rotate from transverse to occiput anterior. Cant be induced if previous Caesar strong contractions against a closed cervix risk of rupture Risk of placenta growing in the scar next time. Only approx 1% of babies infected but approx 50% mortality if infected Perinatal Asphyxia Asphyxia: cessation of gas exchange hypoxia and hypercarbia. Varies from region to region th th 372 4 and 5 Year Notes Reasons for perinatal death: Hypoxia (eg placenta separated, maternal hypertension) Prematurity Congenital abnormality (eg heart defect, spina bifida) Trauma (eg difficult birth) Maternal Death: Death associated with pregnancy or trophoblastic disease up to 3 months after the event (required to be reported to Medical Officer of Health) Causes: Obstetric causes 70%. Eg in anything that causes large uterus twins, polyhydramnios, etc Genital tract trauma during delivery (7%) Coagulation defect Management: Resuscitate mother. Pelvic organ by ~10 days Lochia: red for day 1 3, yellow next 10 days, white until 6 weeks Reproductive and Obstetrics 373 Puerperal Pyrexia = temperature of at least 38 C on any 2 of the first 14 days after abortion or delivery, exclusive of the first 24 hours Incidence: After vaginal delivery: 1 3 % After Caesarean: ~10% Pathogenesis: assume infection until proven otherwise. Can deteriorate quickly need rapid assessment Sources: Clots, retained placenta, etc can facilitate growth Generally an ascending infection Lower genital tract (eg anaerobes). Treat with Pavlik harness Genitals: Check boys for undescended testes (cryptorchidism) 2%, especially if premature, spontaneous descent unlikely beyond 3 months, surgery at 9 12 months. Complete a screening survey such as the Edinburgh Postnatal Depression Questionnaire.
Copyright 2006, Interstate Municipal Gas Agency. IMGA notices will be found posted on the IMGA Downloads page. For problems or questions regarding this Web site contact brubenacker@imga.org.