Clinical Director, University of California, Irvine School of Medicine
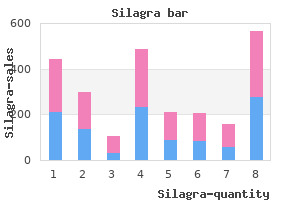
If these features are addressed smoking and erectile dysfunction statistics silagra 100mg on line, the chances of overlooking a sinister cause for headache are greatly diminished erectile dysfunction protocol ingredients order genuine silagra on-line. Their ability to ascribe symptoms to a specific headache on recall may be unreliable erectile dysfunction 43 years old cheap silagra on line. In fact, its clinical diagnosis is based chiefly on the absence of the symptoms that characterize migraine. Although research demonstrates that some criteria are more predictive of migraine than others, no single criterion is sufficient. Many, but not all, patients have other symptoms that they recognize as premonitory. Although nausea is common in migraine patients, vomiting occurs much less frequently. Most migraine patients experience nausea with a large proportion of their headaches, vomiting with a few of their headaches, and neither symptom with some of their headaches. Many migraine patients report never having vomited in association with their headaches. Unilateral pain is a common characteristic of migraine and can be a key symptom in making the diagnosis. However, many migraine patients report headaches that begin bilaterally and then settle on one side or headaches that remain bilateral throughout, but nonetheless meet the other criteria for migraine. Similarly, pulsating or throbbing pain is a common characteristic of migraine but just as many migraine patients will report a penetrating, boring, or stabbing pain. Because approximately 80% of migraine patients also have other headaches and may have more than one headache type at the same time, parsing out migraine symptoms can be challenging. Headache specialists widely believe that moderate-to-severe, recurrent headache is migraine until proven otherwise. Migraine without aura and migraine with aura are distinct clinical entities: a study of four hundred and eighty-four male and female migraineurs from the general population. As experienced clinicians who care for patients know, pattern recognition is an invaluable diagnostic technique in clinical practice, particularly for heterogeneous disorders such as migraine. For example, osmophobia, in addition to photophobia and phonophobia, has been shown to be a highly sensitive and specific feature of migraine. Perhaps one of the challenges migraine patients have is that their headaches present with a host of different signs and symptoms, some of which meet diagnostic criteria for migraine. It is important for patients and physicians to recognize the differences in these headache types so appropriate care is taken regarding treatment. This study evaluated the efficacy of sumatriptan in treating a host of different headache types. Migraineurs with severe disability, as assessed with the Headache Impact Questionnaire score 250 or greater, were enrolled in a randomized, double-blind, placebo-controlled, crossover study. Two hundred forty-nine migraineurs treated 1576 moderate or severe headaches: migraine (n=1110), migrainous (n=103), and tension-type (n=363). This study documents that patients with a diagnosis of migraine also may experience other headache types. Sumatriptan for the range of headaches in migraine sufferers: results of the Spectrum Study. The challenges in sorting through the overlapping features in making a migraine diagnosis are illustrated in this chart. Forty-one percent of male and 51% of female respondents reported receiving a physician diagnosis of migraine.
Adrenoreceptors It is convenient to distinguish several receptor types in explaining the effects of catecholamines erectile dysfunction doctor in los angeles order silagra 50mg with visa. Many more receptor-types can be subtly distinguished by their affinity for different agonists and antagonists and erectile dysfunction otc treatment trusted 50 mg silagra, in even more cases erectile dysfunction ayurvedic drugs in india generic silagra 50 mg without prescription, by their structures. For practical purposes, however, it is probably sufficient to use a classification scheme such as the following: 1. D1, D2, D3, D4, D5 Most people reserve the term "adrenoreceptor" for a1, a2, b1, b2, and b3-receptors. The D receptors are dopamine receptors and are highly relevant to behavior and to Parkinson’s disease and will be treated only briefly in my lectures. The actions of a and ß adrenoreceptors are mediated by diverse intracellular mechanisms. The hormone-receptor ("liganded receptor") interacts with a stimulatory guanine nucleotide-binding regulatory protein (G ), which then activates the adenylyls cyclase. The G regulatory protein sometimes alsoi + ++ interacts with ion channels to activate (K channels) or inhibit (voltage-gated Ca Page 11 Pharmacology 501 January 10 & 12, 2005 David Robertson, M. Many of the most useful agents in clinical medicine act at the level of catecholamine receptors. The indirectly-acting agents (tyramine) elicit their effect primarily by uptake into the postganglionic sympathetic neuron where they displace norepinephrine from cytoplasmic sites and into the synaptic cleft. Because they affect sympathetic neurons throughout the body and because tachyphylaxis occurs they are seldom used clinically, but will be reviewed briefly later. Although catecholamine receptors tend to be most heavily concentrated in the vicinity of neuron terminals, some are located at more distant sites. The nearer a receptor site is to a neuron terminal, the more likely it is to depend on neuronally released catecholamine (usually norepinephrine) for stimulation. The farther a receptor site is from a neuron terminal, the more likely it is that circulating epinephrine and norepinephrine stimulate it. Figure 8: Subgroups of adrenergic agents Page 12 Pharmacology 501 January 10 & 12, 2005 David Robertson, M. Table 1: Autonomic and Adrenoreceptor Effects of Norepinephrine Organ Receptor Response *Medulla Oblongata a2 Reduced sympathetic outflow *Pupil a1 Mydriasis (radial muscle contraction) *Heart b1 Acceleration, contractility increase *Arterioles a1,a2 Constriction *Arterioles b2 Dilation *Veins a1,a2 Constriction Salivary Glands a1,a2 Viscous secretion Pilomotor Muscles a1 Contraction (horripilation, "chill bumps") *Bronchial Muscle b2 Relaxation Gastrointestinal Muscle a1,a2,b2 Relaxation *Uterus b2 Relaxation *Bladder Sphincter a1 Contraction Spleen Capsule a1 Contraction Pancreas a2 Reduced insulin Pancreas ß2 Increased insulin Liver a1,b2 Hyperglycemia Adipose Tissue b1,b3 Lipolysis Adipose Tissue a2 Reduced lipolysis Adipose Tissue b3 Heat production *Kidney b1 Renin release Kidney a2 Sodium conservation, reduced renin *Platelet a2 Aggregation White Blood Cells b2 Demargination *clinically important effect Most agonists and antagonists at catecholamine receptors interact with more than one receptor type. For example, epinephrine (adrenaline) will stimulate a1, a 2, b1, b2 and b3 receptors if given in sufficiently high dosages. Epinephrine has relatively more activity at b2-adrenoreceptors than does norepinephrine. It is advisable to learn the effects of "pure" agonists and antagonists on the various adrenoreceptor types and then learn the adrenoreceptor type specificity of individual drugs. Considerable intellectual effort is required to assimilate adrenoreceptor pharmacology, which constitutes a major category of drug use in man. Since 2000, there has been much new information implicating the autonomic nervous system in the control of both bone and adipose tissue. Sympathetic activation seems to reduce bone mass, whereas reduced sympathetic models have increased bone mass. Sympathetic activation of fat tissues leads to breakdown (lipolysis) whereas parasympathetic activation leads to build up of fat in the abdominal adipose tissue.
Purchase silagra overnight delivery. Erectile dysfunction pills that WORK!.
Know the pathogenesis of edema of congestive heart failure impotence drugs over counter purchase 50 mg silagra mastercard, nephrotic syndrome ayurvedic treatment erectile dysfunction kerala discount silagra 50 mg fast delivery, cirrosis erectile dysfunction drugs and hearing loss purchase silagra 50 mg line, and other clinical conditions 5. Have the basic knowledge about various types of shock, their pathogenesis, manifestations, and complications. Introduction the health and well-being of cells & tissues depend not only on an intact circulation to deliver nutrients but also on normal fluid hemostasis. Edema Definition: Edema is increased fluid in the interstitial tissue spaces or it is a fluid accumulation in the body cavities in excessive amount. Depending on the site, fluid accumulation in body cavities can be variously designated as: a) Hydrothorax – fluid accumulation in pleural cavity in a pathologic amount. Mechanism of edema formation: Approximately 60% of the lean body weight is water, two-thirds of which is intracellular with the remainder in the extracellular compartment. The capillary endothelium acts as a semipermeable membrane and highly permeable to water & to almost all solutes in plasma with an exception of proteins. Proteins in plasma and interstial fluid are especially important in controlling plasma & interstitial fluid volume. Normally, any outflow of fluid into the interstitium from the arteriolar end of the microcirculation is nearly balanced by inflow at the venular end. Edema formation is determined by the following factors: 1) Hydrostatic pressure 2) Oncotic pressure 3) Vascular permeability 4) Lymphatic channels 5) Sodium and water retention We will discuss each of the above sequentially. There are four primary forces that determine fluid movement across the capillary membrane. Each of them can be listed under the above two basic categories, the hydrostatic pressure & the oncotic pressure. The capillary hydrostatic pressure (Pc) This pressure tends to force fluid outward from the intravascular space through the capillary membrane to the interstitium. The interstial fluid hydrostatic pressure (Pif) This pressure tends to force fluid from the interstitial space to the intravascular space. The plasma colloid osmotic (oncotic) pressure (Пp) This pressure tends to cause osmosis of fluid inward through the capillary membrane from the interstitium. The interstial fluid colloid osmotic (oncotic) pressure (Пif) This pressure tends to cause osmosis of fluid outward through the capillary membrane to the interstitium. The plasma oncotic pressure is decreased when the plasma proteins are decreased in various diseases such as: 1. Edema resulting from increased capillary hydrostatic pressure as in the following diseases: 1. Congestive heart failure Clinical classification of edema: One can also clinically classify edema into localized & generalized types. A) Localized B) Generalized 1) Deep venous thrombosis 1) Nephrotic syndrome 2) Pulmonary edema 2) Liver cirrhosis 3) Brain edema 3) Malnutrition 4) Lymphatic edema 4) Heart failure 5) Renal failure Next, we will elaborate on some of the above examples. Reduction of albumin due to excessive loss or reduced synthesis as is caused by: 1) Protein loosing glomerulopathies like nephrotic syndrome 2) Liver cirrhosis 3) Malnutrition 4) Protein-losing enteropathy b. Increased volume of blood secondary to sodium retention caused by congestive heart failure: 65 Fig. Some of these mediators (See the chapter on inflammation) cause increased vascular permeability which leads to loss of fluid & high molecular weight albumin and globulin into the interstitium. Inflammatory edema differs from non-inflammatory edema by the following features a) Inflammatory edema (exudate) ⇒ Due to inflammation-induced increased permeability and leakage of plasma proteins. Therefore, obstruction of lymphatic channels due to various causes leads to the accumulation of the proteinaceous fluid normally drained by the lymphatic channels. In these conditions, the retained sodium & water result in increased capillary hydrostatic pressure which leads to the edema seen in these diseases.
In the workplace icd 9 code erectile dysfunction due diabetes purchase 50mg silagra with visa, primary groups also exist in the form of those who affiliate because of something held in common erectile dysfunction drugs online purchase silagra no prescription. For instance erectile dysfunction questions buy silagra 50 mg cheap, the group members may be all women in the administrative field or all graduates from the same institution, or they may all be of the same ethnic background. These groups are organized around formal rules, procedures, policies and other regulations. The work place is composed of secondary groups that are found in departments or at levels and that form the work group. Formal groups are the official or legitimate work group, while informal groups form for different reasons. The leader must be able to influence both groups and thus move the work group toward meeting its objectives. An effective work group is characterized by the ability to meet its goals through a high degree of appropriate communication and understanding among its members. Another characteristic is the ability to arrive at a balance between group productivity and satisfying individual needs. The leader does not dominate a group like this; instead there is flexibility between the leader and members to use different and individual talents appropriately. This group is cohesive and can 180 Nursing Leadership and Management objectively review its own work and face its problems in a way that balances emotional and rational behavior for a productive group effort. The leader who enhances cohesion and cooperation will be moving the group toward completion of its goals. Characteristics of a Group One of the characteristics of the group is a value structure that is created in groups that comes about because of the influencing process among and between its memberships. For example, some groups value their expertise, they value friendship, or they value higher wages. If the individual violates these norms, he/she will take the risk of being an outcast. Task Behaviors of a Group Some of the available behaviors that participants in the group may exhibit are broadly grouped as task or maintenance behaviors. Task behaviors serve to facilitate and to coordinate group effort in the selection 181 Nursing Leadership and Management and definition of a common problem and in the solution of that problem. Behaviors that fall in this category are: • Initiating-suggests new ideas, or a different way of looking at an old problem, or proposing new activities • Information seeking asks for relevant facts and feelings about the situation at hand • Information giving provides the necessary and relevant information • Clarifying probes for meaning and understanding in whatever the group is considering • Elaborating builds on previous comments and thoughts and thus enlarge the concept under consideration • Coordinating clarifies the relationships among the various ideas and attempts to pull things together • Orienting defines the progress of the discussion in terms of goals to keep the discussion in the right direction • Testing checks periodically to see if the group is ready to make a decision or to recommend some action • Summarizing reviews the content of past discussion 182 Nursing Leadership and Management Maintenance functions are carried out through behavior that maintains or changes the way in which the group is working together. These behaviors seek to allow the group to develop loyalty to one another and to the group as a whole. These roles do not help the group to accomplish its task or to facilitate good member relationships. Phases of Small Groups Orientation Phase: the beginning period in the small group process is called the orientation phase. During this phase, individuals spend time assessing their purpose for joining the group and figuring out where they fit in the group. Members engage in testing the other members and the leader to determine what is appropriate and acceptable behavior within the group. Members spend time at this point trying to identify the nature of the task and the ground rules. Conflict Phase: During this phase, members become less interested in orientation issue, such as how they are fitting into the group, land more interested in control issues, such as how they are influencing the group. Each member wants to be perceived by others as a competent group member with something to offer others. In addition, frequent discussions typically occur 185 Nursing Leadership and Management about what task needs to be completed, which rules of procedure will be followed, and how decisions will be made in the group.
Encourage survivors to actively engage in their pain management plan and to explore options to participate in support groups erectile dysfunction pills from canada generic silagra 100mg overnight delivery. An essential component to this is for the clinician to provide a detailed explanation to the patient on the cause or causes of the pain complaint erectile dysfunction devices diabetes buy discount silagra line. Interagency Guideline on Prescribing Opioids for Pain [06-2015] 50 During active cancer treatment erectile dysfunction treatment raleigh nc generic 100mg silagra overnight delivery, patients may have been accustomed to frequently changing and/or escalating opioid doses with any complaint of worsening pain intensity. Significant education is needed to assist the 9 patient and caregiver to understand this new approach. One study found that 16-73% of breast cancer survivors experience pain, as well as a 308 significant symptom burden of psychological distress and insomnia. The Childhood Cancer Survivor Study reported 11% of adult survivors (mean interval from diagnosis 17 years) 310 experienced medium or higher pain intensity; and 6% of Australian adult cancer survivors at 5-6 years 311 post treatment reported moderate to severe pain. Certain pharmacological therapies can cause lasting pain problems during use, for instance, aromatase inhibitors such as anastrozole, exemestane, and letrozole that are used to prevent recurrence of breast cancer and are taken for variable periods (2-10 years) after completing initial therapy. Nearly half of 313 women using these agents may experience myalgias and arthralgias, which may be of enough 314 severity that 21-38% of patients abandon this potentially life-saving therapy (Table 11). Interagency Guideline on Prescribing Opioids for Pain [06-2015] 51 Chronic cancer-related pain in the survivor can improve significantly with a variety of pharmacological and non-pharmacological therapies. Pain treatments in the survivor should be modeled after chronic non-cancer pain strategies, rather than palliative therapies. In most patients, the primary goal of 315 therapy is functional improvement rather than exclusively a reduction in pain intensity. However, it should be noted that efficacy of these agents has not been established in cancer survivors. Topical agents, such as lidocaine 5% patch, capsaicin cream, or diclofenac gel may be helpful for some post-surgical pain syndromes of cutaneous or myofascial origin. Physical therapy, rehabilitation, and graded exercise programs will help reverse deconditioning and functional loss commonly experienced during cancer treatment. Specialized therapy such as manual lymphatic drainage for lymphedema will improve discomfort from swelling. Counseling for anxiety, depression, and pervasive fear of cancer recurrence is beneficial; as is mindfulness training and other cognitive behavioral strategies to reduce pain. Sleep hygiene education is essential for pain management, as sleep 313 disruption is common in this population. Traditional sleep-inducing agents such as zolpidem are not recommended for long-term use. All new or worsening pain in the cancer survivor must be promptly evaluated to eliminate the possibility of cancer recurrence as the source of pain. Consultation with the patient’s oncologist is recommended to provide guidance as needed. Recurrent or Secondary Malignancy Most survivors struggle with a fear of cancer recurrence, and are well aware that pain may be an initial 313 symptom. The clinician should provide reassurance that all new or worsening pain problems will be assessed and appropriately investigated to eliminate cancer as the cause. Extensive emotional support may be needed, and formal counseling with supportive services may be required to assist with anxiety 300,318 related to the potential for cancer recurrence. The oncologist will direct surveillance screening, either through his/her office, or guide the primary care 319-321 provider through the Cancer Treatment Summary and Survivorship Care Plan. However, it is Interagency Guideline on Prescribing Opioids for Pain [06-2015] 52 essential that all providers involved in the care of cancer survivors know the signs and symptoms associated with cancer, whether from recurrence or secondary malignancy (Table 12).
Copyright 2006, Interstate Municipal Gas Agency. IMGA notices will be found posted on the IMGA Downloads page. For problems or questions regarding this Web site contact brubenacker@imga.org.